Comparison of Imaging Changes and Pain Responses in Patients with Intra- or Extraosseous Bone Metastases Treated Palliatively with Magnetic Resonance- Guided High-Intensity–Focused Ultrasound
Clinical question
Does pain response differ in patients with intraosseous versus extraosseous bone metastases after ablation with MR guided High-Intensity-Focused Ultrasound (HIFU)? Can follow up MR predict treatment response?
Take away point
Patients with intraosseous tumors had significant improvement in pain from baseline after ablation with MR guided HIFU while to those with extraosseous tumors did not. Follow up with MR after ablation with HIFU does not predict efficacy of treatment.
Reference
Giles SL, Brown MRD, Rivens I, et al. Comparison of Imaging Changes and Pain Responses in Patients with Intra- or Extraosseous Bone Metastases Treated Palliatively with Magnetic Resonance-Guided High-Intensity-Focused Ultrasound. J Vasc Interv Radiol JVIR. 2019;30(9):1351-1360.e1. doi:10.1016/j.jvir.2019.02.019
Click here for abstract
Study design
Single arm, prospective study of 21 patients with dominant, painful bone metastasis (9 with intraosseous disease and 12 with extraosseous cortical breach) treated with MR guided HIFU.
Funding Source
Sponsor: Institute of Cancer Research, United Kingdom
Collaborators: Phillips Medical Systems, Cancer Research UK
Setting
Multicenter Study
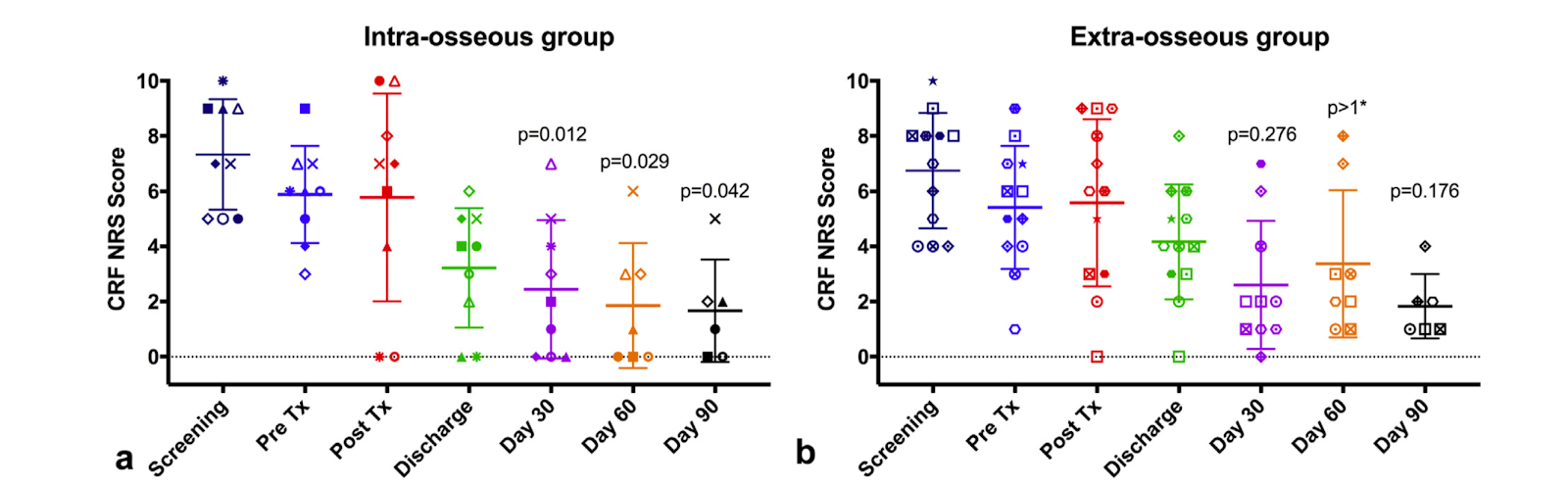
Figure 4
Several scoring systems were utilized by the authors to evaluate post-procedure pain reduction. In this figure, the results of case report forms (CRFs) are shown for treated tumor for (a) 9 patients in the intraosseous group and (b) 12 patients in the extraosseous group. At days 30, 60, and 90 after treatment, scores were significantly lower than those in pretreatment (Pre Tx) for the intraosseous group but not for the extraosseous group.
Summary
High intensity focused ultrasound (HIFU) has shown promising results for palliative treatment of pain from bone metastases potentially related to thermal denervation of periosteum. The authors performed a prospective study of 21 patients with either interosseous or extraosseous painful bone metastasis who were then treated with MR guided HIFU. Gadolinium enhanced T1W images were obtained at the completion of treatment and at 30, 60 and 90 day follow up. Patient pain was assessed using various scoring systems at the time of the procedure and at follow up in addition to recorded analgesic use, which was compared before and after ablation. Patients were categorized as responders and non-responders in regard to post procedure alleviation of pain.A difference from baseline pain was only statistically significant for patients with interosseous tumor on follow up. While 67% of patients with interosseous tumors were classified as responders at 30 days, only 33% of patients in the extraosseous group responded.
While imaging results of the ablated tumor showed nonenhancement in the majority of interosseous tumors, post procedure enhancement patterns of ablated extraosseous tumors varied. There was no difference in follow up imaging enhancement characteristics for patients who were classified as responders or non-responders.
Commentary
The authors in this study evaluated 21 patients with painful bone metastasis after treatment with MR guided High Intensity Focused Ultrasound. While the findings are encouraging for patients with intraosseous disease where the bone cortex remains undisrupted with significant improvement in pain for 67% of their patients at 30 days, results for extraosseous extension of disease were less promising. The authors alluded to the fact that patients with extraosseous disease may have more advanced disease at the time of treatment and more studies evaluating ablative thermal dose per tumor volume in these patients are required. While follow up MR may be beneficial for monitoring disease progression, preliminary results from this study showed that MR could not predict efficacy of treatment. As noted by the authors, in the future, this finding may point to fewer burdensome MRs obtained after ablation.Post Author
Teodora Bochnakova MD
Assistant Professor
Department of Interventional Radiology
Oregon Health and Science University, Portland, OR
@T_bochnakova


