Safety and Effectiveness of Expandable Intravertebral Implant Use for Thoracolumbar Burst Fractures
Clinical question
Are expandable intravertebral implants (Spinejack; Stryker, Kalamazoo, Michigan) a safe and effective treatment option for patients with thoracolumbar spine burst fractures without fracture-related neurologic deficit.Take away point
Expandable intravertebral devices are safe and effective for improving pain, vertebral body height, fracture fragment retropulsion, and central canal diameter compromise in patients without fracture-related neurologic deficit.Reference
Wei H, Hsu D, Katta H, Lowenthal J, Kane I, Kazmi S, Sundararajan S, Koziol J, Gupta G, Johnson S, Kang F, Moubarak I, Roychowdhury S. Safety and Effectiveness of Expandable Intravertebral Implant Use for Thoracolumbar Burst Fractures. J Vasc Interv Radiol. 2023 Aug;34(8):1409-1415.Click here for abstract
Study design
Retrospective, observational, descriptive studyFunding Source
NoneSetting
Single center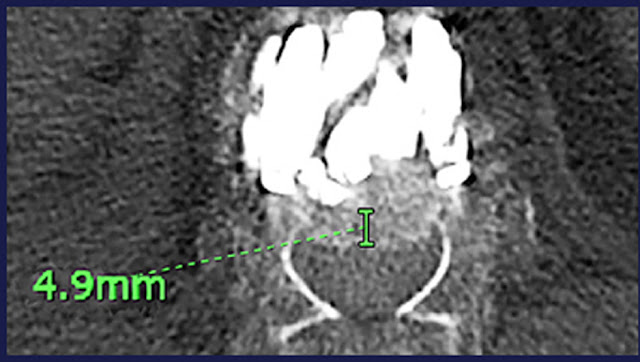
Figure
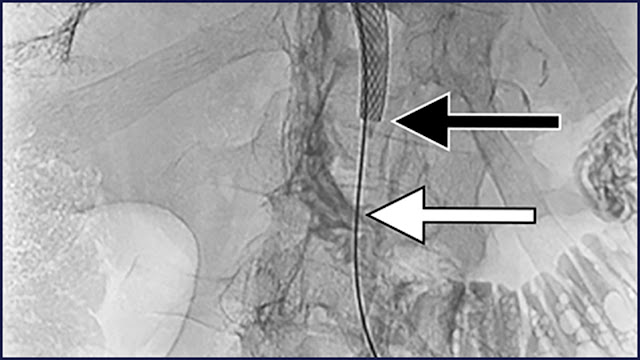
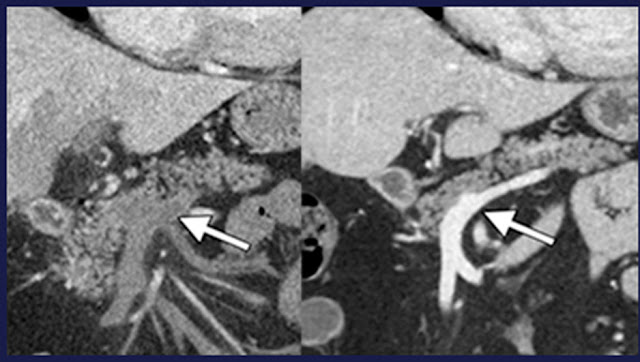
Postprocedural thoracic spine computed tomography using expandable intervertebral implantation demonstrated an improved degree of retropulsion.Summary
Imaging studies before and after expandable intravertebral implantation and medical records of 33 patients, 11 (33.3%) men and 22 (66.6%) women with an overall mean age of 71.7 years ± 8.3, were reviewed for 60 thoracolumbar Magerl Type A3 injuries secondary to osteoporosis, trauma, or malignancy. The mean follow-up time was 299 days.
Implantation of an expandable intravertebral device resulted in a statistically significant reduction in bone fragment retropulsion (mean ± SD, 0.64 mm ± 16.4; P < .001), reduction in the extent of canal compromise (mean, 5.5%; P < .001), increased central canal diameter (mean ± SD, 0.71 mm ± 1.3; P < .001), and restoration of vertebral body height, with a mean increase of 5.0 mm (P < .001). However, the implantation did not result in a statistically significant kyphosis reduction (mean, 1.38°; P = .10). All patients except for 1 reported improvement in pain after surgery, with a mean improvement of 1.54 on a 4-point pain scale (P < .001). No clinically significant adverse events were reported.
Commentary
Expandable, intervertebral implants are a new method of treating vertebral compression fractures. This study evaluates their use in burst fractures that are not causing neurologic deficits. The authors found improvements in pain, central canal compromise, and degree of retropulsion. The authors do admit that the improvements in central canal compromise and retropulsion were small. Kyphosis was not significantly changed after the procedure. This study is a promising early step toward more rigorous comparison of intervertebral implants with vertebroplasty or kyphoplasty in similar settings.
Jefferson Radiology
@IR_Huber
Post author
Timothy Huber, MDJefferson Radiology
@IR_Huber