Transjugular Intrahepatic Portosystemic Shunt and Thrombectomy (TIPS-Thrombectomy) for Symptomatic Acute Noncirrhotic Portal Vein Thrombosis
Clinical question
Is transjugular intrahepatic portosystemic shunt and mechanical thrombectomy (TIPS-thrombectomy) safe and effective for symptomatic acute noncirrhotic portal vein thrombosis (NC-PVT).Take away point
TIPS-thrombectomy is a safe and effective method for treating patients with symptomatic acute NC-PVT.Reference
Shalvoy MR, Ahmed M, Weinstein JL, Ramalingam V, Malik MS, Ali A, Shenoy-Bhangle AS, Curry MP, Sarwar A. Transjugular Intrahepatic Portosystemic Shunt and Thrombectomy (TIPS-Thrombectomy) for Symptomatic Acute Noncirrhotic Portal Vein Thrombosis. J Vasc Interv Radiol. 2023 Aug;34(8):1373-1381.e3.Click here for abstract
Study design
Retrospective, observational, descriptive studyFunding Source
NoneSetting
Single academic center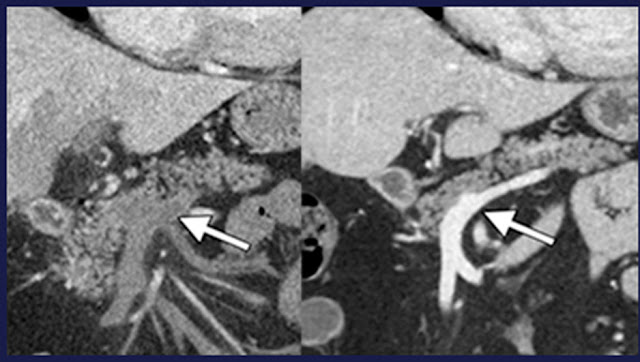
Figure
(Left) Preprocedural coronal reconstruction showed extensive portal, splenic, and mesenteric venous thrombosis (arrow). (Right) Postprocedural coronal image at 1 year showed a well-opacified SMV, splenic vein, and portal vein without evidence of residual thrombosis.Summary
Patients with acute NC-PVT who underwent TIPS-thrombectomy between 2014 and 2021 at a single academic medical center were retrospectively reviewed. Thirty-two patients were included (men, 56%; median age, 51 years [range, 39–62 years]). The causes for PVT included idiopathic (n = 12), prothrombotic disorders (n = 11), postsurgical sequelae (n = 6), pancreatitis (n = 2), and Budd-Chiari syndrome (n = 1). The indications for TIPS-thrombectomy included refractory abdominal pain (n = 14), intestinal venous ischemia (n = 9), ascites (n = 4), high-risk varices (n = 3), and variceal bleeding (n = 2). Variables studied included patient, disease, and procedure characteristics. Patients were monitored over the course of 1-year follow-up.
Successful recanalization of occluded portal venous vessels occurred in all 32 patients (100%). Compared with pretreatment patency, recanalization with TIPS-thrombectomy resulted in an increase in patent veins (main portal vein [28% vs 97%, P < .001], superior mesenteric vein [13% vs 94%, P < .001], and splenic vein [66% vs 91%, P < .001]). Three procedure-related adverse events occurred (Society of Interventional Radiology grade 2 moderate). Hepatic encephalopathy developed in 1 (3%) of 32 patients after TIPS placement. At 1-year follow-up, return of symptoms occurred in 3 (9%) of 32 patients: (a) ascites (n = 1), (b) variceal bleeding (n = 1), and (c) intestinal venous ischemia (n = 1). The intention-to-treat 1-year portal vein and TIPS primary and secondary patency rates were 78% (25/32) and 100% (32/32), respectively. Seven patients required additional procedures, and the 1-year mortality rate was 3% (1/32).
Commentary
In this study of TIPS-thrombectomy for symptomatic, acute, noncirrhotic portal vein thrombosis the authors report significant improvements in patency of the portal system after thrombectomy. They reports a secondary patency rate of 100% at 1 year. These results support the safety and efficacy of TIPS-thrombectomy; however, the study is limited by retrospective nature, small sample size, and short follow up. Longer term follow up, or comparison to anticoagulation alone could be promising future directions.
Jefferson Radiology
@IR_Huber
Post author
Timothy Huber, MDJefferson Radiology
@IR_Huber
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.