Radiation Exposure of Patients and Interventional Radiologists during Prostatic Artery Embolization: A Prospective Single-Operator Study
Summary
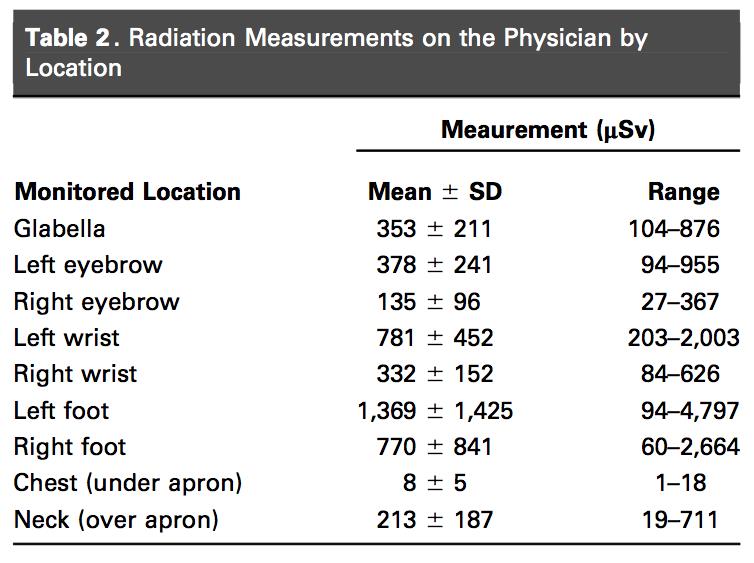
Prostatic artery embolization (PAE) is a technically challenging, often lengthy procedure due to the complex, variable anatomy of the prostatic arteries, which may require multiple views, magnification, and cone-beam computed tomography (CT), all of which contribute to elevated radiation doses to the patient and interventional radiologist. Existing studies on PAE have reported indirect measures of radiation exposure including fluoroscopy times and dose area product (DAP), but none have evaluated direct radiation measures, which are a more accurate assessment of radiation dose. Andrade et al conducted a prospective evaluation of radiation exposure to the patient and practitioner during 25 PAE procedures. Patient peak skin dose (PSD) was measured with radiochromic film, placed under the patient’s hip. Operator radiation dose were attained from 9 pairs of thermoluminescent dosimeters, positioned at various body positions on both sides. All procedures were performed by a single interventional radiologist, whose experience with PAE included completion of a PAE course, assisting with 5 cases, and independent performance of 5 cases. Procedures were performed using an Artis Zee ceiling-mounted angiography system equipped with a flat-panel detector. Ceiling-suspended screen and table curtain were always employed. Fluoroscopy was performed at 15 images/second, digital subtraction angiography performed at 2 images per second. Cone-beam CT was performed only if deemed necessary. Mean patient weight was 71.4 kg (range: 54-88 kg), and prostate volume was 79 cm3 (range: 36-157 cm3). Embolization was performed with 100-200 um polyvinyl alcohol particles or 400-um microspheres to complete prostate artery occlusion. Average fluoroscopy time was 30.9 minutes (range: 15.5-48.3 minutes), with mean total DAP of 451 Gy-cm2 (range: 248-792 Gy-cm2), 75% of which was from fluoroscopy. Mean patient PSD was 2420 mGy (range: 1390-3616 mGy), which is in the range of other complex interventional radiology procedures like transjugular intrahepatic portosystemic shunt, transarterial chemoembolization, and neural embolization. Average effective dose to the practitioner was 17 uSv (range : 4-47 uSv), with higher doses to the left side of the body, including average 0.378 mSv to the left eye. Post-PAE clinical evaluation of patients, including skin check to the lower back and hip, at 15 days, 1 month, and 3 months demonstrated no sequelae of radiation exposure.
Commentary
PAE is known to be a challenging procedure that may require lengthy fluoroscopy times and high radiation exposure, even in the hands of experienced practitioners. As more interventional radiologists undertake this complex procedure, it is essential to elucidate the degree of associated radiation exposure to patients and operators. In prior PAE series, the degree of radiation exposure has been reported through indirect measures, which may be inaccurate surrogates for direct measures of radiation dose. The direct measures of radiation dose assessed by Andrade et al therefore provide a unique and important addition to the PAE evidence base. For operators, the PAE exposure levels of average 17 uSv were similar to other complex interventional radiology procedures, highlighting the importance of optimizing radiation protection techniques and equipment when performing PAE. Although no patients developed skin radiation injury in this series, the mean patient PSD of >2 Gy with range up to 3.6 Gy, in combination with prior case reports of radiation dermatitis following PAE, suggest that vigilant clinical follow-up is merited. These high radiation doses are particularly relevant considerations for patients who undergo repeat PAE for whom attempts should be made to distribute the dose to a different skin region. Although this study was subject to biases of being a small, single center series with all cases performed by a single interventional radiologist, these results provide an important foundation to our understanding of radiation exposure during PAE. Reduction of these radiation exposure levels will be important aims for further refinement and maturation of PAE for the treatment of benign prostatic hyperplasia.
Click here for abstract
Andrade G, Khoury HJ, Garzón WJ, Dubourcq F, Bredow MF, Monsignore LM, Abud DG. Radiation Exposure of Patients and Interventional Radiologists during Prostatic Artery Embolization: A Prospective Single-Operator Study. J Vasc Interv Radiol 2017; 28:517-21.
Post Authors:
Jeffrey Forris Beecham Chick, MD, MPH, DABR
Assistant Professor of Vascular and Interventional Radiology
Vice Quality Assurance and Safety Officer
University of Michigan Health Systems
Michigan Medicine
James X. Chen, MD
Resident in Radiology
Hospital of the University of Pennsylvania
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.