Balloon Guide Catheter in Endovascular Treatment for Acute Ischemic Stroke: Results from the MR CLEAN Registry
Clinical question
Compare the outcomes after endovascular treatment for acute ischemic stroke with and without the use of a balloon guide catheter.
Take away point
Balloon guided catheters are associated with higher reperfusion grade, early improvement in neurologic status, and lower rates of symptomatic ICH. However their use has no positive effect on long-term functional outcome.
Reference
Goldhoorn, Robert-Jan B., et al. Balloon Guide Catheter in Endovascular Treatment for Acute Ischemic Stroke: Results from the MR CLEAN Registry. Journal of Vascular and Interventional Radiology, Volume 30, Issue 11, 1759-64
Click here for abstract
Study design
Retrospective review of data collected during the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in The Netherlands (MR CLEAN).
Funding source
None
Setting
Medical centers participating in the MR CLEAN trial in the Netherlands.
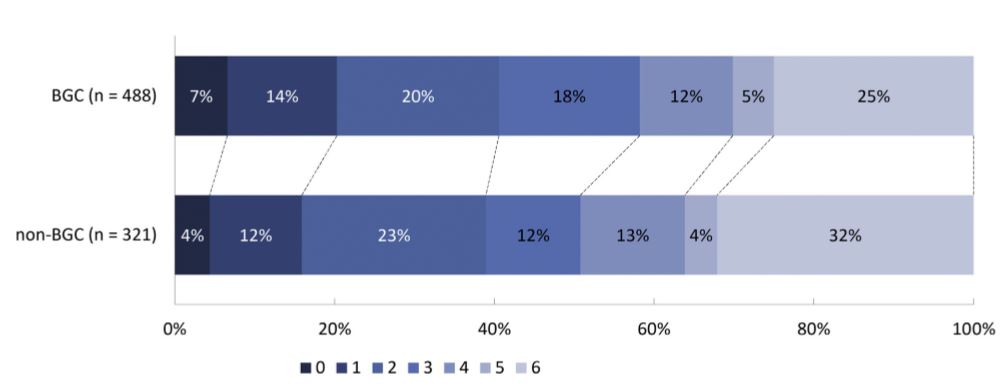
Figure 2. Functional outcome on the mRS (modified Rankin Score) for patients treated with BGC (balloon guide catheter) vs non-BCG for acute ischemic stroke intervention.
Summary
Endovascular treatment of acute ischemic stroke has been shown to improve patient outcomes. Multiple endovascular methods have been developed to remove the acute thrombus from the occluded vessel. Currently it is operator depending on the technique used to re-vascularize the ischemic segment of tissue. These include mechanical clot disruption (stent retriever) with and without flow arrest, aspiration thrombectomy, local thrombolytic infusion and a combination of these techniques. Flow arrest is obtained by using a balloon guide catheter or in cases of high grade carotid stenosis it occurs when a sheath is placed across the stenotic lesions. The authors used data from the MR CLEAN trial and compared patients long-term functional outcome, eTICI score (reperfusion grade) and HIHSS score 24-48 hours after intervention.
All the patients were part of a randomized control trial and underwent endovascular treatment for acute ischemic stroke. Balloon guide catheters (BGC) were used in 538 patients (60%) and 359 patients (40%) had intervention without BGC. The individual operator technique was not discussed in this paper since it was looking at data from a RCT, which had numerous operators throughout the Netherlands.
The primary outcome was modified Rankin Scale (mRS) score at 90 days. The secondary outcomes were reperfusion grade after treatment (eTICI) and National Institutes of Health Stroke Scale (NIHSS) score after 24-48 hours.
The use of logistic regression was used to adjust for age, sex, prestrike mRS score, NIHSS score, collateral grade, and time from onset to EVT.
The percentage of functionally independent patients at 90 days was similar between the 2 groups (41% vs 39%; P- 0.64). BGC significantly improved eTICI (acOR, 1.33; 95% CI, 1.04-1.70) and reperfusion (eTICI grade =/> 2B) in the BGC group (75%) vs the non-BGC group (68%) with a P = 0.02. NIHSS score was lower in patients treated with BGC (9 vs 11, P – 0.06) with an improvement of 4+ points more frequently (62% vs 52%; P < 0.01). After adjusting for confounders the use of BGC had a decreased death rate (23% vs 29%, P = 0.03).
Commentary
The authors retrospectively evaluated data from a national RCT for acute ischemic stroke to see if the use of balloon guide catheters (BGC) had a better outcome. They found that there was no difference in 90 day functional outcome of patients when comparing the two endovascular techniques. They did find that patients who had endovascular revascularization with a BGC had better early improvement in NIHSS scores and better reperfusion grades (eTICI).
It is very difficult to directly apply the study results to daily stroke practice. The use of BGC didn’t improve 90 day functional outcome; however it did result in early patient improvement. I think it would be interesting to study how this effects resource utilization. Patients that improve quickly after a stroke can be stepped down to a lower level of care and return home earlier, which may benefit their overall well-being and decrease hospital cost. I don’t think this will result in decreased utilization of balloon guide catheters in stroke treatment; however, further studies need to be done to confirm or disprove these findings.
Post Author
Hasnain Hasham, MD
Interventional Radiology Fellow
Dotter Interventional Institute
Oregon Health and Science University, Portland, OR
@irhasham
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.