Embolization versus Surgery for Stabilized Patients with Solid Organ Injury
Clinical question
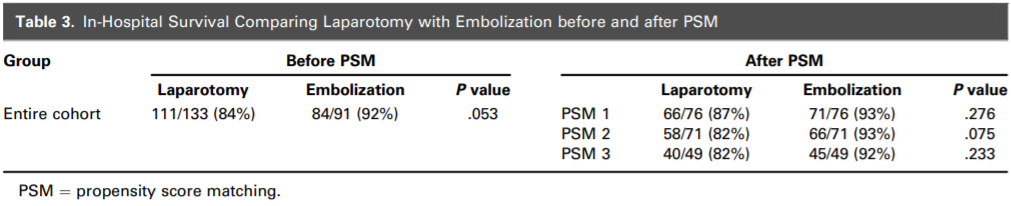
Compare the in-hospital survival after embolization versus laparotomy in hemodynamically unstable patients who responded to resuscitation and initial CT identified isolated solid organ injury.
Take away point
No significant difference was seen between in-hospital survival in those receiving embolization versus laparotomy.
Reference
Embolization versus Surgery for Stabilized Patients with Solid Organ Injury. Aoki, M.. et al. Journal of Vascular and Interventional Radiology, Volume 32, 1150-1155.
Click here for abstract
Study design
Retrospective cohort study from the Japan Trauma Data Bank between 2004-2018.
Funding Source
No funding
Setting
Multi-center.
Figure
Summary
Hemorrhage in the setting of trauma is often successfully managed surgically or with embolization depending on the clinical scenario and resources available. Currently, embolization is recommended for hemodynamically stable patients with solid organ injury, while surgical management is recommended for patients with hemodynamic instability. Those who respond to initial resuscitation may be appropriate for embolization. This study compares in-hospital survival following embolization versus laparotomy in hemodynamically unstable patients with solid organ injury who respond to initial resuscitation.
This is a retrospective cohort study performed in Japan between 2004-2018 using the Japan Trauma Data Bank. Patient selection included: patients over the age of 15, completion of abdominal CT, liver and/or splenic injury, sBP <90mm Hg and received a blood transfusion within 24 hours. Patient exclusion included: severe abdominal injury (AIS >3), except for splenic or liver injuries, AIS of 6, dead on arrival, administration of CPR and aortic cross-clamping. Patients were then divided into groups based on having received laparotomy or embolization (see figure above). The primary outcome was in-hospital survival. Secondary outcomes included, complications, length of hospital stay, percentage of patients discharged to home, and rate of splenectomy. Notable analysis technique included propensity score matching analyses, comparing the following models: original cohort (PSM1), cohort minus the penetrating mechanism (PSM2), and cohort adjusted by the time to transfusion and to treatment (PSM3).
Of the baseline characteristics, there were significant differences in sex, sBP, GCS and ISS in PSM 1 and 2, and GCS in PSM3. There was no significant difference between laparotomy and embolization in the 3 propensity score matching models regarding in-hospital mortality, liver injury, splenic injury, time to treatment or analyzed complications. Notable limitations include lack of information on which organ was embolized, their definition of hemodynamic instability and possible confounders not included in their PSM analysis. In addition, the authors note a high degree of access to CT scanners and a short time to embolization. This may be due to CT scan and embolization availability in many of the OR suites in Japan included in this study.
Commentary
Regardless of OIS scores, this study demonstrates no significant difference in in-hospital mortality between laparotomy and embolization in stabilized patients who had received a CT scan. This data helps underscore the utility of endovascular techniques in trauma, particularly those that may be deemed hemodynamically unstable. The authors define instability as a sBP <90 mm Hg and having received a blood transfusion. The American College of Surgeons defines hemodynamic instability “as global or regional perfusion that is not adequate to support normal organ function”. They also note that relying on sBP is not sufficient, due to multiple compensatory mechanisms that exist to prevent hypotension. Overall, hemodynamic instability is often a gestalt, which is challenging to define by objective numbers. Additionally, although there is high availability of CT scans in Japan, the inclusion criteria of having received a CT scan often suggests some element of stability.
The greatest challenge is the applicability of these findings in healthcare settings where access to CT may be limited or prompt endovascular treatment may be logistically challenging. In this study, patients had timely access to both imaging and endovascular treatment. Time to treatment is immensely important in trauma patients, therefore care should not be delayed to pursue an endovascular option. If the patients by definition are hemodynamically unstable, the facility should have access to hybrid operating rooms or the ability to rapidly transfer to surgical management. In the US, the majority of hospitals are not level 1 trauma centers, and are often able to surgically manage patients more quickly. In the correct clinical and healthcare setting, these findings demonstrate endovascular treatments are an appropriate treatment option in the unstable trauma patient. Future research noting specific organ embolization and treatment techniques may help establish protocols and help guide clinical decision making.
Post Author
Marissa Stumbras, MD
Interventional Radiology Resident, PGY3
Oregon Health & Science University
@MarissaStumbras
Edited and formatted by @NingchengLi
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.