Identification of Parameters Influencing the Vascular Structure Displacement in Fusion Imaging during Endovascular Aneurysm Repair
Clinical question
Can we safely perform a zero-contrast procedure relying solely on fusion imaging? What contributes to renal ostia displacement by the insertion of a stiff system during endovascular aneurysm repair (EVAR) of abdominal aortic aneurysm (AAA)?
Take away point
Sharper angulation between aneurysm neck and sac results in decreased fusion imaging accuracy and precludes EVAR deployment without contrast validation.
Reference
Identification of Parameters Influencing the Vascular Structure Displacement in Fusion Imaging during Endovascular Aneurysm Repair. Lalys F. et al. Journal of Vascular and Interventional Radiology (JVIR), Volume 30, Issue 9, 1386-1392.
Click here for abstract
Study design
Single arm, prospective, cohort study of 50 patients undergoing EVAR.
Funding Source
No reported funding
Setting
Academic hospital, University Rennes, France.
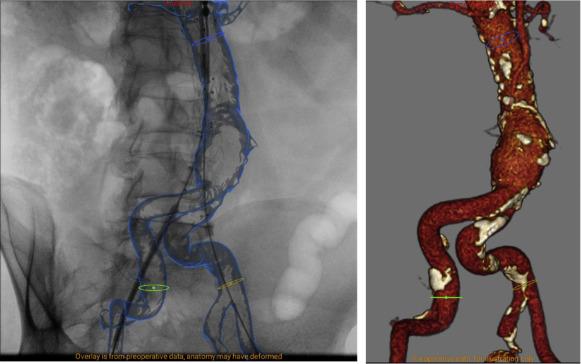
Figure 1
EndoNaut station main screen visualization during an EVAR procedure, with the fusion overlaid on the fluoroscopic image on the left and the corresponding 3D visualization on the right.
Summary
Fusion imaging technology has been shown to decrease contrast usage and radiation dose in both standard and complex endovascular aneurysm repair (EVAR) of abdominal aorta aneurysm (AAA). However, its relevance is limited by deformation of vascular structures after insertion of stiff devices during the procedure. The authors performed a prospective study of 50 patients undergoing EVAR to quantify the displacement of the lowest renal artery ostium and to identify the contributing anatomical parameters.Patients included in this study were adults undergoing EVAR, who were not open-repair candidates, had AAA diameter greater than 50 mm, or had AAA growth rate greater than 10 mm per year. Patients were excluded if a fenestrated or branched endograft was used, or if the repair was performed for ruptured AAA.
EndoNaut station was used for fusion workflow. Digital subtraction angiogram performed intra-procedurally after insertion of stiff devices but prior to EVAR deployment was compared with the fusion roadmap generated pre-operatively using CT angiography. A large number of anatomical parameters were measured, including tortuosity index, length, diameter, angulation, calcification, thrombus, and distance to spine of the relevant vascular segments. Sharpest angulation, as defined by Van Keulen et al, was also calculated.
Mean displacement of the lowest renal artery ostium was 4.1 ± 2.4 mm (range, 0–11.7 mm), with a left/right displacement of 1.6 ± 1.7 mm (range, 0–6.9 mm) and a craniocaudal displacement of 3.5 ± 2.4 mm (range, 0–11.3 mm). Sharpest angulation between the aneurysmal neck and sac contributed significantly to the accuracy of fusion imaging (p = 0.00001).
Commentary
The authors in this study quantified the degree of renal artery ostia displacement after insertion of stiff devices during EVAR. They further identified the sharpest angulation between the aneurysmal neck and sac as a significant contributor in fusion imaging accuracy. The findings support the need for better fusion imaging technology with semi-automatic intra-procedural adjustments, especially in EVAR cases with significant angulation between the aneurysmal neck and sac. The paper also underlines the importance of small-amount contrast injection prior to EVAR deployment for confirmation of major vascular ostia. Future fusion imaging technology with more adaptive intra-procedural capability, potentially with the assistance of artificial intelligence, should be validated in a similar manner with prospective design and anatomical analysis before we proceed to attempt a zero-contrast EVAR deployment.Post Author
Ningcheng (Peter) Li, MD, MS
Integrated Interventional Radiology Resident, PGY-3
Department of Interventional Radiology
Oregon Health and Science University, Dotter Interventional Institute
@NingchengLi