Middle Meningeal Artery Embolization with Liquid Embolic Agents for Chronic Subdural Hematoma: A Systematic Review and Meta-analysis
Clinical Question
Is middle meningeal artery embolization (MMAE) via liquid embolic agents a safe and effective alternative to conventional neurosurgery for treating chronic subdural hematomas?Take Away Point
MMAE demonstrated 100% success rate, significantly lower reoperation, recurrence, and mortality rates compared to conventional neurosurgery.Reference
Mowla A, Abdollahifard S, Farrokhi A, Yousefi O, Valibeygi A, Azami P. Middle Meningeal Artery Embolization with Liquid Embolic Agents for Chronic Subdural Hematoma: A Systematic Review and Meta-analysis. J Vasc Interv Radiol. 2023;34(9):1493-1500.e7. doi:10.1016/j.jvir.2023.05.010Click here for abstract
Study Design
Systematic review and meta-analysis of 14 studies containing 276 patientsFunding Source
No reported fundingSetting
Academic, Keck School of Medicine, Los Angeles, CAAcademic, Shiraz Research Center for Neuromodulation and Pain, Shiraz, Iran
Academic, Shiraz University of Medical Sciences, Shiraz, Iran
Academic, Fasa University of Medical Sciences, Fasa, Iran

Figure
Figure E1.Heterogeneity, proportion, and 95% confidence interval related to the success rate of chronic subdural hematoma treatment following middle meningeal artery liquid embolization after excluding the study by Fan et al. CI = confidence interval. (Fan G, Wang H, Ding J, et al. Application of absolute alcohol in the treatment of traumatic intracranial hemorrhage via interventional embolization of middle meningeal artery. Front Neurol 2020; 11:824.)Summary
The authors performed a systematic review and meta-analysis. Initially, 628 studies were retrieved using Preferred Reporting Items for Systematic Reviews and Meta-Analyses Criteria. The researchers ultimately extracted 14 eligible articles comprising of 276 patients undergoing 305 embolization procedures. They then evaluated the clinical success rate, adverse events rates, recurrence rates, reoperation rate, and reduction in size of cSDH.
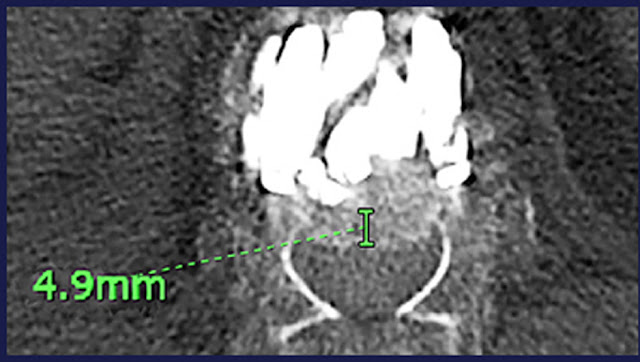
The results of the study demonstrated the following: Mean age of 66 years, 100% technical success rate, 1% adverse event rate, 3% recurrence rate, 4% reoperation rate, 94% reduction rate in the size of the hematoma, 78% achieving complete elimination of the hematoma, 0% mortality rate. All of these results were within the 95% confidence interval.
These results demonstrated highly favorable results when compared to invasive neurosurgical interventions. For example, the article demonstrated that the recurrence rates of common neurosurgical techniques ranged from 11.7-28.1% compared to MMAE’s 3%. The reoperation rate with conventional methods was up to 26.4% compared to to MMAE’s 4%.
Commentary
Post author
Naeem Patel, DORadiology Resident, PGY4
Department of Radiology, Interventional Radiology Division
Hartford Hospital, Hartford, CT
@Naeemp7Patel